NOTE: I've moved this blog post to my professional website, EyeDock. More importantly, I've written an update, Changes in Plaquenil Risk Calculations based on new recommendations based on a 2014 study. The calculator has also been updated to reflect these changes.
As all eye care providers should be aware, there have been some revisions in the recommendations of how we monitor our Plaquenil patients secondary to two articles1,2 published earlier this year.
Whenever I want a quick review of Chloroquine and Hydroxychloroquine retinotoxicity I always head to Ron Melton and Randall Thomas's excellent website, Eyeupdate. As expected, their site has been updated with the new recommendations and I won't bother duplicating their efforts here.
I will, however, plunge a little deeper into some of the dosaging concerns they brought up in their article. After all, I never met an algebraic equation I didn't like, and I have a obsession for looking at data and trying to establish trends. In addition, I thought I might be able to create a simple calculator to help my fellow eye care professionals determine their patient's retinotoxic risk as it relates to plaquenil dosage. It's not that the calculations are particularly difficult, but, being Americans and using the moronic English system of measurements, it's requires a few more steps than a busy doctor should have to take.
Going forward, I'm going to limit my discussion to hydroxychloroquine (Plaquenil) and women. Chloroquine is less common, and men are less likely to be taking these medications. Besides, the trends for men and Chloroquine will be very similar to what I discuss here.
Let's dive in. Melton & Thomas describe the typical safe Plaquenil dosage this way:
The usual dosage is two 200mg tablets per day. This is generally a "safe" dose for patients having a lean body weight of at least 135 lbs. The generally-regarded safe dosage is 6.5mg/kg/qd, thus the 135 lb. safety threshold.
I think it's helpful to break down where this 135 lb threshold is coming from. First, let's convert the body weight to kilograms:
135 lbs x 0.45359237 Kg / lb = 61.2 kg
Then multiply the body weight and the "safe"daily dosage.
61.2 kg x 6.5mg/kg/qd = 398 mg/qd ---> ~two 200 mg tablets
To further visualize this, here it is in graphical form:

The blue line represents the generally-regarded safe daily dose per pt's weight (using the 6.5mg/kg/qd). For individual's below 135 lbs the safe dosage falls below 400mg/qd, and, as a consequence, the typical dosage of two 200mg tablets carry a greater risk of retinotoxicity.
However, things get a little more complicated when we take into account obesity. Again, from Melton & Thomas's Web site:
We stress here that HCQ is not absorbed into adipose tissue. This means that an obese person who weighs 160lbs may be considered within the "safe" zone, but their lean body weight may be only 120lbs, which poses an increased relative risk. We have communicated this critical issue of lean body weight to our referring rheumatologists and dermatologists, and have asked them to assess the lean body weight of each of their HCQ patients and make this information known to us, so that we can more accurately assess the risk for retinotoxicity . . .
I thought it would be helpful for my calculator to include the option of calculating lean body weight for overweight individuals. The formulas for lean body weight are as follows:
Lean Body Weight (men) = (1.10 x Weight(kg)) - 128 ( Weight2/(100 x Height(m))2)
Lean Body Weight (women) = (1.07 x Weight(kg)) - 148 ( Weight2/(100 x Height(m))2)
I went ahead and built a calculator to
- take a patient's height and weight and calculate lean body weight
- take the lean body weight and calculate the "safe" HCQ dosage
Unfortunately every set of numbers I plugged in indicated that my patient would be at a high risk dosage if they were taking 400 mg/day. For example, let's take a 160 lb 5'4" woman:
160 lbs x 0.45359237 Kg / lb = 72.5 kg
5'4" = 64 inches --> 64" * 0.0254 meters / inch = 1.625 meters
Lean body weight = (1.07 x 72.5kg) - 148 ( 72.5kg2/(100 x 1.625)2) = 48.2kg
48.2 kg x 6.5mg/kg/day = 313 mg / day
For this patient it appeared that the typical 400mg/day dosage would be too high. I tried various other weights and heights and found that very few combinations resulted in a safe daily dosage above 400mg. Again, I decided to plot this:
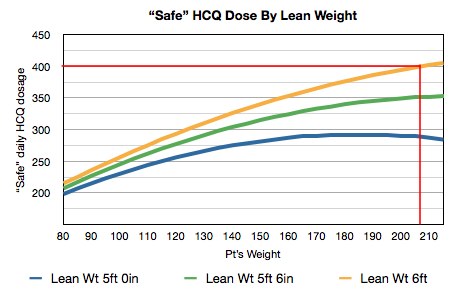
After taking the patient's weight and using their height to calculate the lean mass, the "safe" daily dosages were calculated. According to this graph, all but 6 foot tall 207lb women should be at risk for retinotoxic effects with 400mg daily dosages of plaquenil.
As this is ridiculous, and has no relation to what we see in the real world, we've obviously made a bad assumption here. If we define lean body weight as the body mass minus the body fat, well, we're always going to end up with a significantly smaller weight than a person's "real" weight, even for individuals at their ideal weight. Multiplying this low number by our "safe" dosage will always result in a small recommended dosage, and obviously the 6.5mg/kg/qd wasn't meant for this. Perhaps there is a conversion factor for safe dosage per kg of lean body weight, but, if there is, I haven't come across it.
This prompted me to re-read Revised Recommendations on Screening for Chloroquine and Hydroxychloroquine Retinopathy.2 This paper states:
Chloroquine and [Plaquenil] are not retained in fatty tissues, so patients who are obese could be seriously overdosed if medicated on the basis of weight alone. Obese individuals should be dosed on the basis of height, which allows estimation of an asthenic or "ideal" body weight...
Aha - they're referencing ideal body weight, not lean body weight. Ideal body weight is calculated with the following formulas:
Ideal Body Weight (men) = 50 + 2.3 ( Height(in) - 60 )
Ideal Body Weight (women) = 45.5 + 2.3 ( Height(in) - 60 )
As such, our 5'4" female would have an ideal body weight of:
5'4" = 64 inches
45.5 + 2.3 (64 - 60) = 54.7 kg
And a "safe" daily plaquenil dose of:
54.7 kg x 6.5mg/kg/qd = 356 mg / qd
So, for this patient it appeared that the typical 400mg/day dosage would still be too high. Let's look at another graph:

Now we're comparing the patient's ideal weight, calculated from their height (note that this does not take into account the pt's true weight), and again calculating the "safe" daily dosage. Interestingly, this indicates that a woman needs to be taller than 67 inches (5'7") before the 400mg/day dosage becomes a lower risk. As the average woman is shorter than this height it would seemingly indicate that 400mg/day may be a high risk dose for the average woman. However, this doesn't ring true as the typical dosage is 400mg/day and is considered to be appropriate for most individuals.
This made me curious about the disparity between dosing based on height (and calculating the ideal weight) or based solely on weight. If every person is at their ideal weight it won't make any difference, but how about for overweight or obese individuals? First, let's define "overweight" and "obese" - the Word Health Organization defines these terms based on the Body Mass Index (from Wikipedia):
BMI
Classification
< 18.5
underweight
18.5–24.9
normal weight
25.0–29.9
overweight
30.0–34.9
class I obesity
35.0–39.9
class II obesity
≥ 40.0
class III obesity
... where BMI = weight (kg) / height (m) 2
Let's take our 5'4" woman from above and see what she would weigh if she were "overweight" or "obese". I'll arbitrarily choose the lower end of the range listed in the BMI table above (overweight BMI = 25). So, we know that our 5'4" woman is 1.625 meters tall. We'll plug that number into the above equation to see what weight would give us a BMI of 25:
25 = w / 1.6252
w = 25 * 1.6252 = 66.02 kg
Again, calculating "safe" daily plaquenil dosage for this weight:
66.02 kg * 6.5 mg/kg/qd = 429 mg
As expected, it indicates a higher "safe" dosage (429 vs 356mg) than the calculation using ideal body weight for this height.
For the last time, let's graph this relationship to get a look at the big picture:

In this graph, the lowest line represents the ideal weight, which was calculated by the height. The other two lines use the method above to calculate a weight that is equal to a BMI of 25 (overweight) or 30 (Obese I) for each height. This effectively illustrates how assessing risk based on true weight alone would predict a much higher "safe" dosage than determining the acceptable dosage based on ideal weight (which, in turn, is based solely on the patient's height).
In the end what have we learned here? Not very much, I'm afraid, at least not anything we didn't already know. We obviously have to be aware of our patient's plaquenil dosage, especially in our overweight patients. For overweight individuals it is helpful to use ideal body weight (based on height), rather than true weight, although it's not clear how overweight a person needs to before you switch formulas. Furthermore, ideal weight calculations seem to suggest a lower "safe" dosage than might be expected.
Also, it's important to understand I've taken a couple general recommendations here and tried to extrapolate more information than I have a right to. The Marmor2 article states:
A significant percentage of the reported HCQ toxic cases have been associated with daily doses > 6.5mg/kg . . .
which tells us 6.5 mg/kg is an appropriate guideline to follow but isn't necessarily a mathematical absolute, just like we know that not everyone who has an IOP above 24mmHg has glaucoma and that everyone below 18mmHg does not.
In addition, we cannot get too obsessed with daily dosages as other risk factors for retinotoxicity exist. In fact, the cumulative dosage is thought to be a more significant risk factor, to the point where the incidence of HCQ retinotoxicity is less than 1% within the first 5 years of medication use. Other risk factors include renal or liver disease, age, preexisting macular disease, and possibly genetic factors.
Despite the fact that 1) there may be some gray areas in Plaquenil dosage calculations and 2) daily dosage is not the only risk factor, it is a risk factor that the eye care specialist can assess. Again, the calculations are not especially difficult, but I hope I can make them a little easier for the busy practitioner.
1 Michaelides, M., et al. "Retinal Toxicity Associated with Hydroxychloroquine and Chloroquine." Arch. Ophthalmic. Vol. 129, No. 1 January, 2011
2 Marmor, M. F., et al. "Revised Recommendations on Screening for Chloroquine and Hydroxychloroquine Retinopathy." Ophthalmology, Vol. 118, No. 2, February, 2011